TCM para aumento de pênis
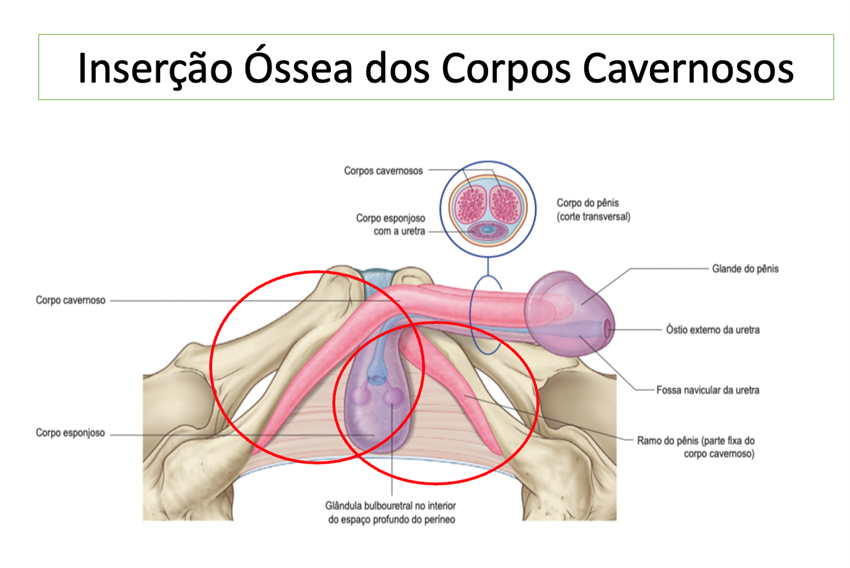
O pênis tem uma porção visível e outra que se localiza na região perineal. Há uma porção fixa, ligada ao osso, num segmento chamado de tuberosidade isquiática. A técnica de “Total Corporal Mobilization”(TCM) visa liberar todo o seguimento fixo do pênis, fazendo com que o toda a estrutura do pênis seja mobilizada para a superfície, aumentando o tamanho do pênis.
Entre as indicações para a realização do TCM, incluem-se o micropênis, o pênis amputado e a reconstrução genital no homem trans. Situações outras, excepcionais, podem ser beneficiadas pelo método, após avaliação pelo profissional.
A figura ilustra a anatomia do pênis e os seguimentos circulados em vermelhos representam a parte fixada no osso, também chamada de crura.
A técnica está publicada no https://pubmed.ncbi.nlm.nih.gov/35838516/ onde pode-se acessar um vídeo demonstrativo
Learn about the reconstructive surgery techniques criated by Dr. Ubirajara
TCM for penis enlargement
The penis has a visible portion and another in the perineal region. A fixed portion is attached to the bone in a segment called the ischial tuberosity. The “Total Corporal Mobilization” (TCM) technique aims to release the entire fixed segment of the penis, causing the entire structure of the penis to be mobilized to the surface, increasing the size of the penis.
Indications for performing TCM include micropenis, amputated penis, and genital reconstruction in trans men. Other, exceptional situations can benefit from the method, after evaluation by the professional.
The figure illustrates the anatomy of the penis and the segments circled in red represent the part attached to the bone, also called the crura.
The technique is published at https://pubmed.ncbi.nlm.nih.gov/35838516/ where you can access a demonstrative video.
Corporoplastia para redução do clitoris
A hipertrofia ou aumento do clitoris pode ocorrer por várias razões, principalmente pelo aumento dos níveis sanguíneos da testosterona. Eventualmente, o clitoris aumenta sem uma razão específica, também chamada de idiopática. As causas mais frequentes são a hiperplasia adrenal congênita e o uso exógeno de testosterona para fins estéticos.
O aumento do clitoris pode gerar uma série de desconfortos emocionais que podem culminar na disfunção sexual feminina. Muitas referem ter vergonha de se despirem na frente do parceiro ou da parceira e de usar biquini pela marca do genital.
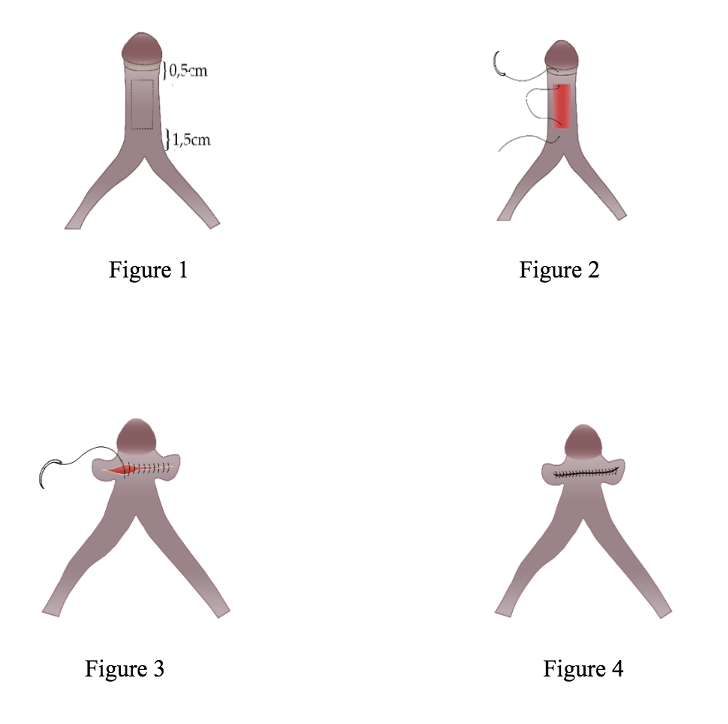
As técnicas de redução do clitoris realizadas até o momento necessitam a dissecção (descolamento) do feixe vascular e nervoso que vão até a glande e a excisão (retirada) dos corpos cavernosos. Como consequência há um risco aumentado de formigamento da glande ou de comprometimento vascular. Além disso, o clitoris tem ereção e a retirada dos corpor cavernosos faz com que não haja mais tumescência do clitoris na excitação.
O Dr. Ubirajara idealizou uma técnica já publicada (ubmed.ncbi.nlm.nih.gov/35263057/), que visa simplificar a cirurgia, não sendo necessária a dissecção dos nervos e vasos e onde é possível preservar a ereção clitoridiana (veja desenho abaixo). Essa técnica é uma modificação da técnica de Hodson publicada nos anos 90, porém se compara favoravelmente pelo melhor aspecto cosmético.
Corporoplasty for clitoris reduction
Hypertrophy or enlargement of the clitoris can occur for a number of reasons, most notably an increase in blood levels of testosterone. Eventually, the clitoris enlarges without a specific reason, also called idiopathic. The most frequent causes are congenital adrenal hyperplasia and the exogenous use of testosterone for aesthetic purposes.
Enlargement of the clitoris can generate a series of emotional discomforts that can culminate in female sexual dysfunction. Many women are ashamed of undressing in front of their partner and wearing a bikini because of the mark on their genitals.
So far, the clitoral reduction techniques require the dissection (detachment) of the vascular and nervous bundle that goes to the glans and the excision (removal) of the corpora cavernosa. Consequently, there is an increased risk of glans tingling or vascular compromise. In addition, the clitoris has an erection, and the removal of the corpora cavernosa means that there is no longer any tumescence of the clitoris in arousal.
The Doctor. Ubirajara devised a previously published technique (ubmed.ncbi.nlm.nih.gov/35263057/), which aims to simplify the surgery, not requiring nerve and vessel dissection and where it is possible to preserve the clitoral erection (see drawing below). This technique is a modification of the Hodson technique published in the 1990s, but it compares favorably for its better cosmetic appearance.
Duplo retalho in e onlay para estenose de uretra
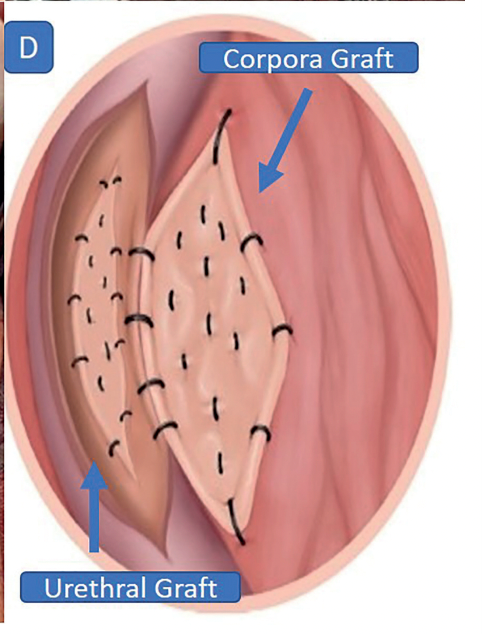
A estenose de uretra é tratada, na sua maioria, por procedimento cirúrgico, a uretroplastia. Nos estreitamentos longos, a mucosa da boca é o tecido mais utilizado para alargar a uretra, com alta taxa de sucesso. Porém, quando a uretra é muito fina, o uso de apenas um segmento é insatisfatório e a técnica de duplo enxerto, como proposta por Palminteri et al., é a alternativa.
Um possível problema da técnica de Palminteri é a colocação do enxerto na porção anterior da uretra, não havendo um suporte tecidual para nutrir e ajudar na fixação do enxerto.
Na técnica idealizada pelo Dr Barroso (https://pubmed.ncbi.nlm.nih.gov/33848080/), o segundo enxerto é colocado inlay, ou seja, no próprio segmento estreitado, dando um suporte para uma melhor “pega”do enxerto. Veja a figura.
Double flap in and onlay for urethral stenosis
Urethroplasty is the procedure of election for the treatment of urethral stenosis. In long strictures, the oral mucosa is the tissue most used to widen the urethra, with a high success rate. However, when the urethra is very thin, using only one segment is unsatisfactory and the double graft technique, as proposed by Palminteri et al., is the alternative.
A possible problem with the Palminteri technique is the placement of the graft in the anterior portion of the urethra, as there is no tissue support to nourish and help with graft fixation.
In the technique devised by Dr Barroso (https://pubmed.ncbi.nlm.nih.gov/33848080/), the second graft is placed inlay, that is, in the narrowed segment itself, providing support for a better “grip” of the graft. See the figure.
U invertido para cirurgia de hipospadia
Nos casos onde a hipospadia é perto do escroto, a cirurgia precisa ser realizada em dois tempos, sendo o primeiro de enxertia e o segundo para a reconstrução uretral. No primeiro tempo, muitos pacientes necessitarão a colocação de enxertos para retificar o pênis e pavimentar o tecido que será a uretra no futuro. Esse tecido muitas vezes é a mucosa do lábio ou bochecha. Esse tecido é escolhido pela similaridade com o tecido uretral e por não deixar cicatrizes visíveis na área doadora.
O problema de cada enxerto é a sua contração, que na uretra gira em torno de 20%. Por isso, em algumas situações, nova enxertia precisa ser utilizada. Na técnica idealizada pelo Dr. Barroso, uma extensão maior de tecido é retirada e enxertada num formato de U invertido, dobrando o tamanho do enxerto e, portanto, reduzindo as chances de retração. Essa técnica está publicada no link: https://pubmed.ncbi.nlm.nih.gov/18996051/
Inverted U for hypospadias surgery
In cases where the hypospadias is close to the scrotum, the surgery must be performed in two stages, the first for grafting and the second for urethral reconstruction. In the first stage, many patients will need grafts to straighten the penis and pave the tissue that will be the urethra in the future. This tissue is often the mucosa of the lip or cheek. This tissue is chosen because of its similarity to the urethral tissue and because it does not leave visible scars in the donor area.
The problem with each graft is its contraction, which in the urethra is around 20%. Therefore, in some situations, a new graft needs to be used. In the technique devised by Dr. Barroso, a larger extension of tissue is taken and grafted in an inverted U shape, doubling the size of the graft and therefore reducing the chances of retraction. This technique is published at the link: https://pubmed.ncbi.nlm.nih.gov/18996051/